
Pareto Insights: Medicare Advantage Payment Year 2024 Model Update (v28)
Summary
This month, CMS released the “Advance Notice of Methodological Changes for Calendar Year (CY) 2024 for Medicare Advantage (MA) Capitation Rates and Part C and Part D Payment Policies”. This release included, among other items, major changes to the MA risk adjustment model from risk adjustment MA model v24 to proposed risk adjustment MA model v28. Pareto Intelligence has reviewed these model changes and has estimated the potential impact for health plans.
Model Changes
With the proposed implementation of v28, Centers for Medicare and Medicaid Services (CMS) would increase the number of diagnostic Hierarchical Conditions Categories (HCCs) from 86 (in v24) to 115 (in v28 proposed). This change comes with a significant decrease in the number of International Classification of Diseases (ICD-10) codes that map to those 115 HCCs. Under the v24 model, CMS utilizes 9,797 ICDs, compared to just 7,770 in the proposed v28 model.
CMS explains that it reviewed conditions where coding variation in MA was higher relative to Medicare Fee-For-Service (FFS) with its clinical experts to identify conditions with discretionary coding variation. In accordance with Risk Adjustment Model Principle 10, discretionary diagnostic categories that are “particularly subject to intentional or unintentional discretionary coding variation or inappropriate coding by health plans/providers, or that are not clinically or empirically credible predictors of future expenditures, should not increase cost predictions” should be excluded from prospective payment models.
In addition to this, CMS added HCC constraints to the diabetes and congestive heart failure disease categories. In proposed model v28 the coefficients of the HCCS within these categories will carry the same weight.
- Constrained all Diabetes HCCs (HCC 36, 37, and 38)
- Constrained Congestive Heart Failure HCCs (HCCs 224, 225, and 226)
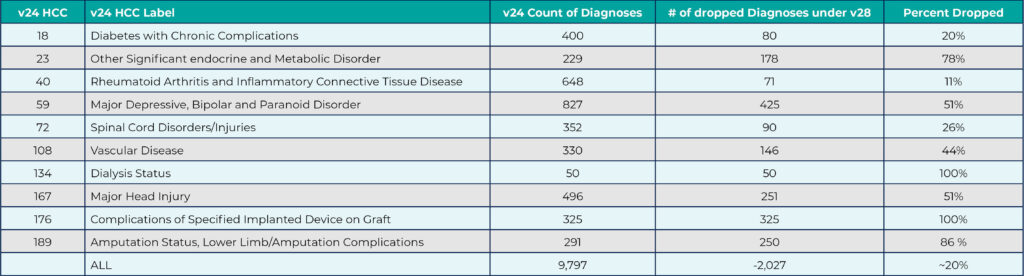
Some of the HCCs are noticeably more affected than others by the number of dropped ICD-10 codes from the model. The table below highlights the notable changes in the number of unique ICD-10 codes dropped under the v28 model:
Estimated RAF Impact
Per CMS, “The CY 2024 impact on MA risk scores of the proposed Part C CMS-HCC model, is projected to be -3.12%, which represents a $11.0 billion net savings to the Medicare Trust fund in 2024."
Utilizing 2022 dates of service for Community Non, Partial, and Fully dual members (CN, CP, CF), Pareto analyzed the differences between v24 and v28 models for MA enrollees. Prior to applying coding intensity and normalization factors, the proposed v28 MA model is resulting in a RAF decrease in the range of 7% to 22% with an average of 13%. After applying the updated FFS Normalization Factor, the RAF impact of the proposed v28 model is +2 to -14% with an average of -4%.
Using an average of 11 coverage months and $750 premium amount, this RAF decrease translates into an average $418 Per-Member-Per-Year (PMPY) decrease in annual risk adjusted premiums.
Impact Drivers
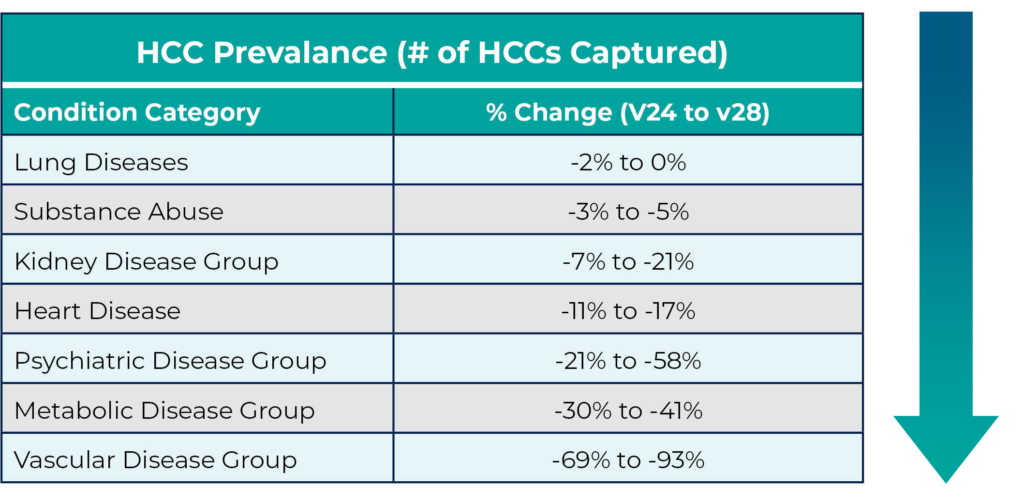
The table below shows the change in prevalence for captured HCCs under each model across some of the most prevalent HCC categories within Medicare Advantage. These changes are driven by the overall decrease in the number of ICDs utilized in the proposed v28 model.
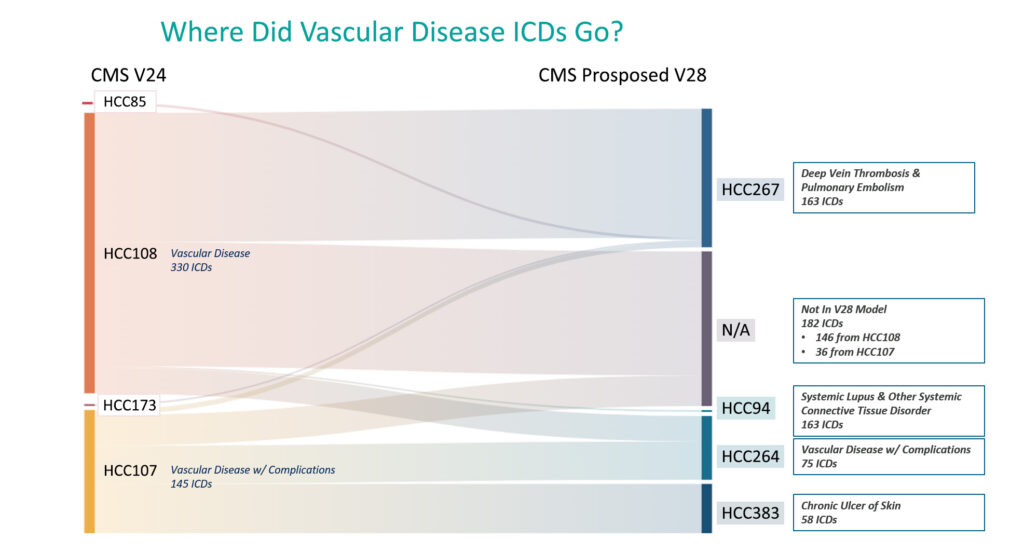
Vascular Disease
Vascular disease is by far the most impacted HCC, with over 82% average decline in the number of HCCs mapped under the v28 model. This decline appears to be driven by two main factors:
- v28 significantly decreased the number of ICD codes mapping to vascular disease (formerly HCC108, now HCC264). Under v24, 330 ICDs mapped to HCC108 (vascular disease) and 145 ICDs mapped to HCC107 (vascular disease with complications). Of those ICDs, 182 are no longer represented in the proposed v28 model. In one population, this decrease in ICDs accounted for over 98% of the reduction in the number of HCCs mapped.
- “Two-for-one” ICDs have been removed from the MA Model. Under the v24 model there were five ICDs that mapped to both HCC18 (diabetes with complications) and HCC108 (vascular disease). Under v28, one of those five has been removed and the remaining four map only to HCC37 (diabetes with complications).
Diabetes
While the volume of diabetes HCCs captured under the proposed v28 model remains unchanged compared to v24, a major proposed change is found in the diabetes coefficient values. All diabetic conditions will have the same coefficient, regardless of severity. Using the community, non-dual, aged variables, the table below provides an example of this:

While plans will likely see a similar prevalence of diabetes conditions under the proposed v28 model, this proposed change, specifically related to HCC37 (previously HCC18) will result in additional RAF decrease.
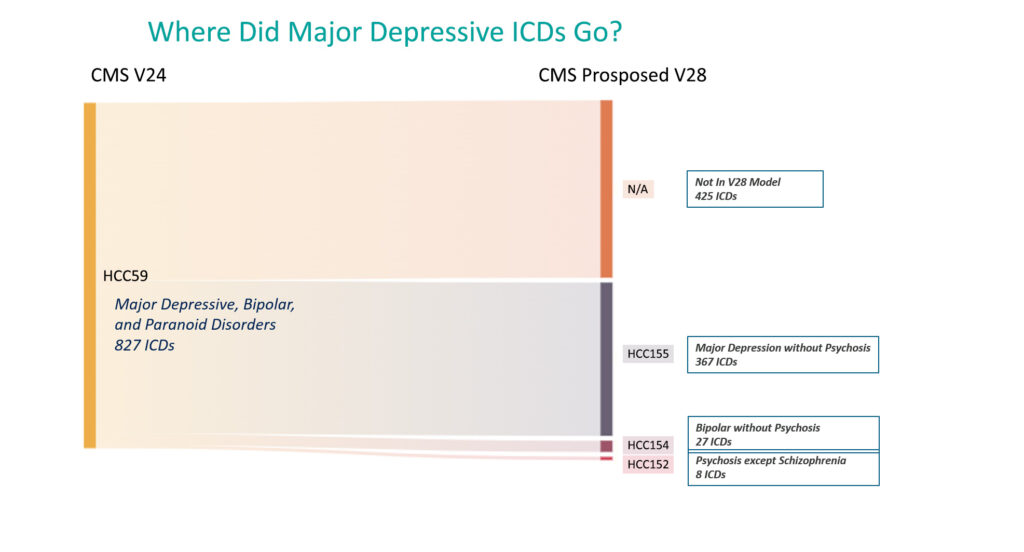
Major Depressive
Similar to vascular disease, over 50% of the ICDs mapping to HCC59 (Major Depressive & Bipolar Disorder) have been completely removed from the proposed v28 model.
Retrospective Chart Reviews
Health plans should consider the impact on ICD codes identified from supplemental sources, like chart reviews. For example, if a single source code is identified and added under v24, that would no longer apply in v28. This ICD may not be included in the v28 proposed model—how much is the plan’s chart review campaign and overall RAF impacted? Coding teams that are accustomed to coding charts through the lens of v24 may need to evaluate how v28 impacts coding practices. Moving from v24 to the proposed v28 model will surely add a new level of complexity while completing multiple years of retrospective and prospective activities simultaneously.
If you have questions about these proposed CMS v28 model changes, the impact to your population, or would like to review your current strategy, reach out to us below.